How is high value in health care defined?
The health care sector is characterised by conflicting interests that often vary based on the stakeholder; including access to services, profitability, high quality, cost containment, safety, convenience, patient-centeredness, and satisfaction.
The overarching goal, however, should be high value for patients – value being defined as health outcomes achieved per Euro spent. Improving value is the most effective, reliable way to drive system progress and benefit both provider and recipients of health care. Because the value of health care is measured in results and not inputs, the quality and effectiveness of any given treatment, and its availability at a fair price, is of greater importance than a crude measure of the overall volume of treatment available. Therefore, we suggest a two pronged approach to improving efficiency and value: first, we must optimise services, and second, optimise costs.
Ensuring quality of services
Any assessment of value must be holistic – meeting a range of different criteria that depend on the patient’s medical condition, as well as factors relevant to the carers involved. Different conditions – e.g. a diabetic child or a trauma victim – may require very different assessments of value.[1] With this in mind, physicians should follow this holistic approach and, ideally, have a team of specialists focusing on issues related to medical treatments (e.g. psychological help for parents of a chronically ill child, but also cost effective treatment options to not financially overburden parents).
However even if areas for improvement can be recognised, it is not always easy to implement changes. Improving health care is closely linked with management and leadership development. As frontline health care providers, physicians are increasingly in need of basic managerial and leadership skills. The increasing risk in current practice, however, is that the decision-making processes in hospital organisations are instead dominated by non-physician hospital administrators. (2) Physicians, on the other hand, have been trained to recognise signs and symptoms of diseases and know which therapy options and/or lifestyle changes can alter the course of a disease. What they lack is the implementation of cost-effective management options. Nevertheless, as the patient is at the centre of all considerations (whether cost-effective or not), the treating physician should be at the core of the decision-making process.
Optimising costs
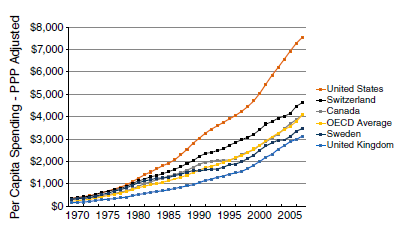
The increasing growth in total health expenditure per capita is a worldwide issue, as shown in Figure 1, and is detrimental to value. It is at largely rooted in three physician-driven occurrences: 1) Preventable or avoidable hospital (re)admissions; 2) inappropriate or non-beneficial treatment; and 3) overuse or misuse of diagnostic testing. (3) All of these three cost pressures will also act to lessen the value of care – inconveniencing the patient with unnecessary treatments and investigations, and heightening concerns about minor or non-existent health problems.
HOW DOES THIS AFFECT CHILDREN?
Children rarely have a voice of their own when it comes to choosing their treatment options. They are dependent on parents, as well as physicians, to advocate for their interests and their well-being. This means that non-medical parents should ideally be advised by medical specialists in order to make the right decisions for their child. Besides their medical expertise, these medical specialists should also be trained in high-value cost-conscious care (HVCCC) practices. This would prevent the instrumentalization of children for cost effectiveness- or other management reasons.
In addition to this, there should be more awareness-raising and funding opportunities for orphan diseases. Since these mainly affect children, saving costs in “regular” medicine can indirectly contribute to more funding for research and treatment of rarer diseases.
PROGRAMS AVAILABLE
The simplest way to reduce costs is to raise awareness of unnecessary interventions to ensure that investigations and treatment are both cost effective and useful.
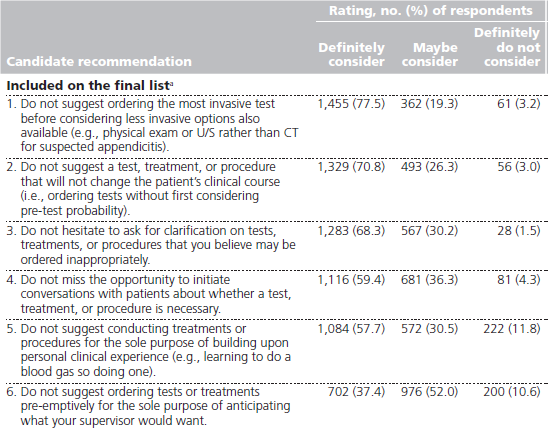
The “Choosing wisely” initiative, which had its beginnings in USA, Canada, and Australia, is an excellent example of this. Specialists were surveyed to determine which measures they considered cost ineffective or, in more extreme cases, useless. From the answers received, a short list of the most important items were selected to help future specialists make valuable, patient-centred decisions. Figure 2 shows an example from the Australian Choosing Wisely list for paediatricians.

But efforts within the healthcare community to raise awareness cannot end with creating a list for residents and/or fellows – they must to start earlier on. Studies show that physicians’ behaviour develops early on in training and that the medical education environment helps shape behaviour (4,5). For this reason, Choosing Wisely Canada (CWC) has created a survey and distributed it amongst students, to create a list for medical education underlined by clinical vignettes, highlighting behaviours to avoid (see Figure 3).
Figure 3: Six Things that Medical Students and Trainees Should Question – Choosing Wisely Canada (CWC) (6) (Source: Lakhani, Anand; Lass, Elliot; Silverstein, William K.; Born, Karen B., PhD; Levinson, Wendy, MD; Wong, Brian M., MD, FRCPC (2016) “Choosing Wisely for Medical Education: Six Things Medical Students and Trainees Should Question”, in Academic Medicine, Https://journals.lww.com/academicmedicine/fulltext/2016/10000/Choosing_Wisely_for_Medical_Education___Six_Things.19.aspx#)
The hope remains that these recommendations also have an impact on faculty, as they strongly influence the cultural and behavioural norms in medical education that affect learning about the careful management of limited resources (stewardship).
Given that, and as some of the recommendations are challenging to follow without guidance from the faculty, CWC has launched the STARS (Students and Trainees Advocating for Resource Stewardship) movement – an initiative that lends legitimacy to the student voice. Two students of each medical school in Canada were invited to leadership training and asked to launch student movements at their respective schools, with the goal of enacting change and raising the profile of resource stewardship in medical training. (6)
However, simply training the students and hoping for faculty members to catch on is likely to fail on its own. Many of these initiatives also include formative programs for the trainers in order to guarantee substantial change. As students, it is important to be taught to communicate wisely and effectively with patients and caregivers about unnecessary tests – especially when confronted with patients and family members who might demand them in search of reassurance. It is therefore crucial that healthcare professionals learn to communicate that such measures can actually expose patients to potential harm and have a negative impact on the health system by contributing to rising healthcare costs. (7)
OUR RECOMMENDATIONS
Terms like High Value Cost Conscious Care (HVCCC) and Choosing Wisely programs need to become an integral part of medical studies and postdoctoral training programs if we are to ensure high value in health care. As healthcare professionals, we should always share the overarching goal of shifting from doctor- or institution-centred health care to patient-centred health care, while developing better training for physicians in management and leadership skills. With a comprehensive approach focused both on mitigating costs and ensuring quality services, our system will be better equipped to give patients the care they deserve.
Young EAP and EAP recommend that healthcare professionals choose investigations and treatments based on clinical need and the likelihood of the test result changing their decision making. Decision making should be based upon clinical need and not upon the motives of non-clinical managers. We would advocate for leadership training to be included in Paediatric training to help Paediatricians develop these skills. EAP and Young EAP are currently working on creating a Choosing Wisely list for Europe and are hoping for contribution from as many European doctors as possible.
About the authors:
List of Authors
Andreas Trobisch is member of Young EAP. He is a paediatric trainee at the University for Pediatric and Adolescent Medicine in Graz, Austria.
Sian Copley is a 4th year resident from the UK working in the North East of England. Sian represents UK paediatric trainees within Young EAP, and paediatric trainees/Young EAP within the EAP Advocacy Group.
Robert Ross Russell is the chair of the European Board of Paediatrics and a member of the Executive Committee of the European Academy of Paediatrics. He is a Consultant Paediatrician at Cambridge University Hospitals Foundation Trust in the UK.
References

New ways to test high-risk medical devices.
Manufacturers of medical devices need to test their products before being allowed to market them. Specifically, they require clinical data showing their medical device is safe and efficient. In this context, the EU-funded CORE-MD project will translate expert scientific and clinical evidence on study designs for evaluating high-risk medical devices into advice for EU regulators. The project will propose how new trial designs can contribute and suggest ways to aggregate real-world data from medical device registries.
It will also conduct multidisciplinary workshops to propose a hierarchy of levels of evidence from clinical investigations, as well as educational and training objectives for all stakeholders, to build expertise in regulatory science in Europe. CORE–MD will translate expert scientific and clinical evidence on study designs for evaluating high-risk medical devices into advice for EU regulators, to achieve an appropriate balance between innovation, safety, and effectiveness. A unique collaboration between medical associations, regulatory agencies, notified bodies, academic institutions, patients’ groups, and health technology assessment agencies, will systematically review methodologies for the clinical investigation of high-risk medical devices, recommend how new trial designs can contribute, and advise on methods for aggregating real-world data from medical device registries with experience from clinical practice The consortium is led by the European Society of Cardiology and the European Federation of National Associations of Orthopaedics and Traumatology, and involves all 33 specialist medical associations that are members of the Biomedical Alliance in Europe.