
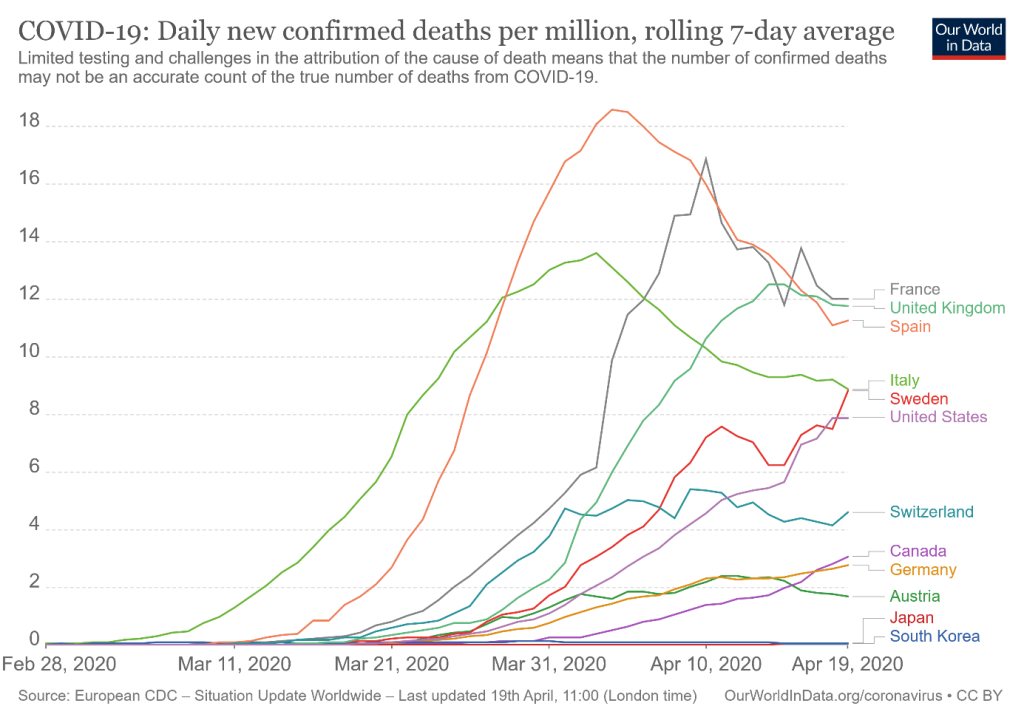
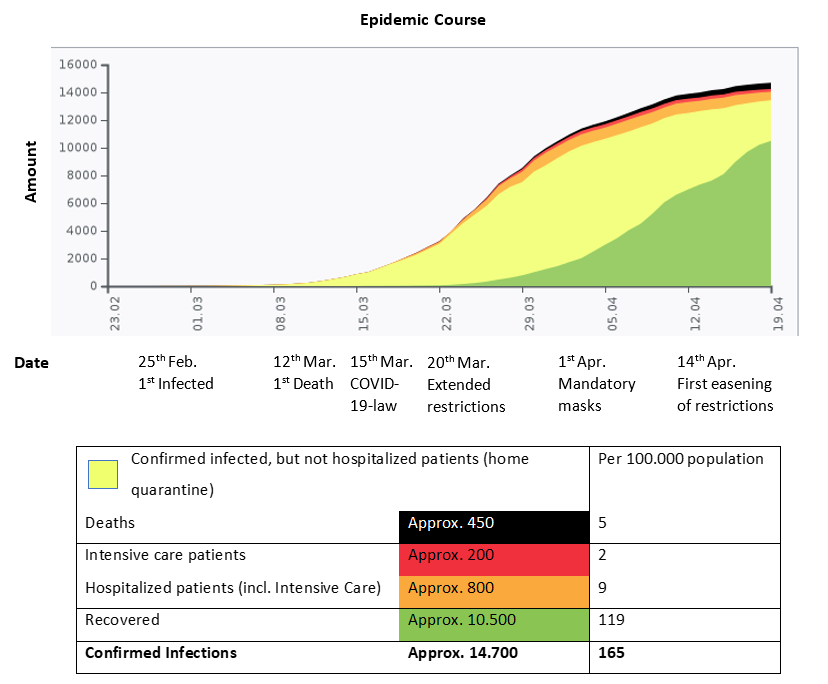
On 25th of February 2020, Austria confirmed the first two cases of COrona VIrus Disease 2019 (COVID-19), a couple from Lombardy, Italy. (1) In the following days more patients were tested positive for Severe Acute Respiratory Syndrome CoronaVirus 2 (SARS-CoV-2) (2). On 12th of March 2020, Austria confirmed the first death of COVID-19, a 69-year-old man from Vienna died in Vienna’s Kaiser-Franz-Josef Hospital (3). By 13th of March 2020, there were 422 confirmed cases (4), by 14th of April 2020 14.713 confirmed cases and 452 death cases (5). Death cases were defined as death in association with COVID-19 (not necessarily causal).
COVID-19 was classified as notifiable infectious disease to enable prompt action of health authorities. Already having observed the outbreaks in Asia and Italy, the Austrian government decided to act fast even though evidence was lacking and released the first order regarding COVID-19 on 28th of February 2020. The first COVID-19 law was released on 15th of March 2020 and followed by further laws, several orders and regulations (6). Areas were put in quarantine when increased transmission had occurred to stop further spread. Dramatic restrictions were introduced, further ones were added and existing ones prolonged. Initial restrictions included closing of all universities and schools, cancelling of all outdoor events with more than 500 people and all indoor events with more than 100 people as well as several travel restrictions. Employers were called to enable home office. Further, a ban was announced for public gatherings of more than five people and all gastronomy (except delivery restaurants) and shops not selling essential goods were closed.
Nationwide, homes were only allowed to be left for one of the following four reasons (7):
In addition, from early on several recommendations and containment measures were introduced to the public comprising the reduction of social contacts and introduction of physical distancing, instructions how to wash hands and how to sneeze and cough. The population was repeatedly asked to stay at home in order to „flatten the curve“. The recommendation for the population to wear masks when entering supermarkets, doctors’ offices, public buildings or public transport followed later.
The Austrian government conducted regular press conferences to inform the public. Media played a major role in distributing information about COVID-19. Numerous newspaper articles and broadcasts on internet, television and radio were published to alert the population about the seriousness of the situation. The enormous information flood with partly contradictory messages might have also contributed to some extent to uncertainty among the population.
Restrictions were accepted by the population in about 95 %. People not following the rules were frequently fined by the police (8).
To date (20th of April 2020) it seems that the Austrian response has worked and the spread of Covid-19 is „under control“ with a health care system that is not occupied to its full capacities. (Figure 1, 5). The current data suggest that children in Austria are hardly affected and hospital admissions of children due to COVID-19 are rare.
Early restrictions allowed the health care system to have time and get prepared in setting up diagnostic facilities and logistics like separating COVID and non-COVID treating facilities in hospitals but also to train health care workers in the correct use of personal protective equipment (PPE). All non-urgent appointments including medical and surgical interventions were postponed.
Challenges during the response included timely supply of PPE for health care workers across Austria especially in primary care settings and getting information about positively tested patients to the treating doctors. There was also a short discussion about installing nationwide tracking systems but as yet, general resistance by the population has prevented this approach.
Some confusion was caused among the population and doctors by a first announcement that all vaccinations and well-child-visits should be postponed for 3 weeks. One day later the Austrian government recommended to enable routine vaccinations especially in infants under strict safety precautions.
Since April 14th 2020 the government has advised a stepwise easening of restrictions. At this timepoint several questions remain open: Will the stepwise easening work or will numbers explode later? What economic, psychological and social effects will we see in the near future and long term? How will children be affected in respect of home schooling and reduction of social contacts? Will we observe increased vaccine gaps or delayed diagnoses of impairments and diseases in children?
To address these questions the Austrian government agreed on financial support for employers and employees. Several institutions started helplines to tackle psychological and social problems. The Austrian Society of Paediatrics and Adolescent Medicine pointed out the importance of scheduled health checks, in particular developmental checks and routine vaccinations in children.
About the authors:
List of Authors
Daniela S. Kohlfürst (Austria) – is a member of Young EAP and Young ESPID and chair of the national junior society of paediatrics and adolescent medicine in Austria. She is a paediatric trainee at the Medical University of Graz, Austria.
Andreas Trobisch (Austria) – is a member of Young EAP and Young ESPID. He is a general paediatrician, subspecializing in neonatology and infectious diseases at the Medical University of Graz, Austria.
Hans Juergen Dornbusch (Austria) – is a member of EAP and ESPID. He is chair of thce EAP vaccination working group. He is a general paediatrician in primary care and associate professor of paediatrics at the Medical University of Graz, Austria.
References

New ways to test high-risk medical devices.
Manufacturers of medical devices need to test their products before being allowed to market them. Specifically, they require clinical data showing their medical device is safe and efficient. In this context, the EU-funded CORE-MD project will translate expert scientific and clinical evidence on study designs for evaluating high-risk medical devices into advice for EU regulators. The project will propose how new trial designs can contribute and suggest ways to aggregate real-world data from medical device registries.
It will also conduct multidisciplinary workshops to propose a hierarchy of levels of evidence from clinical investigations, as well as educational and training objectives for all stakeholders, to build expertise in regulatory science in Europe. CORE–MD will translate expert scientific and clinical evidence on study designs for evaluating high-risk medical devices into advice for EU regulators, to achieve an appropriate balance between innovation, safety, and effectiveness. A unique collaboration between medical associations, regulatory agencies, notified bodies, academic institutions, patients’ groups, and health technology assessment agencies, will systematically review methodologies for the clinical investigation of high-risk medical devices, recommend how new trial designs can contribute, and advise on methods for aggregating real-world data from medical device registries with experience from clinical practice The consortium is led by the European Society of Cardiology and the European Federation of National Associations of Orthopaedics and Traumatology, and involves all 33 specialist medical associations that are members of the Biomedical Alliance in Europe.

