
Interconnected care has for some time now made its way to the minds of people thinking about the future of modern healthcare. The concept of interconnected care has become widely used when policymakers and other stakeholders in care services are planning for the future of modern healthcare. The main problem is that the term interconnected care is too broad to be self-explanatory. This article aims to bring you closer to an understanding of both what the concept means, why it is increasingly important to incorporate in healthcare and also give some examples of what this looks like in pediatric care.
In 2009 WHO released a first report on Systems Thinking (1), which is the general idea underlying the concept of Interconnected care. Interconnected care is about linking every aspect of healthcare, ensuring that professionals and individuals have access to all the information and available services they need for an ideal treatment of patients (2). It is a tool that is meant to help us improve healthcare by creating a linkage and common understanding among the different stakeholders involved in providing healthcare. The most used clinical term for this is to ‘ensure a common understanding’- or a ‘shared goal’ for the provided care.
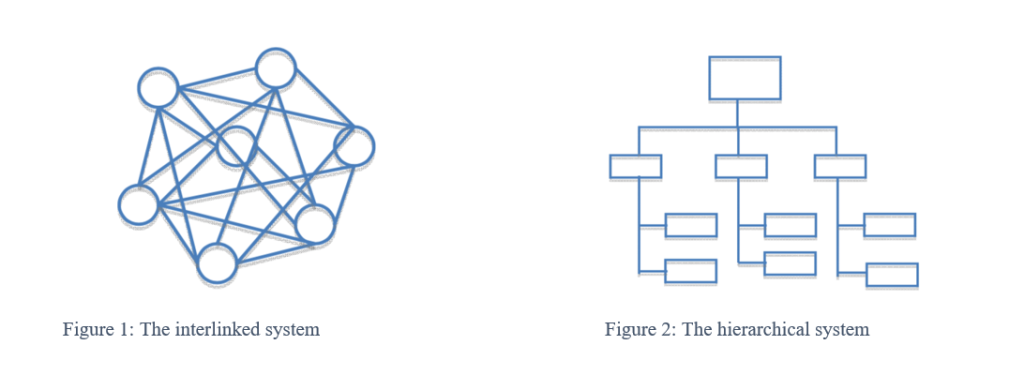
Visually you can imagine Interconnected care as a map that shows you involved stakeholders and how they are connected with each other. This stands in contrast, but not in dualism to, the traditional hierarchical form of providing healthcare services. Both models are shown underneath: in Figure 1 the interlinked system, in Figure 2 the hierarchical system (3). You can think of healthcare as a very complex machinery that only when having both systems working co-dependently will function at its’ most efficient.
USING THE METHOD OF ‘THE GOLDEN CIRCLE’ (4) TO EXPLAIN THE CONCEPT OF WHY, HOW AND WHAT
The underlying WHY of Interconnected care is that this approach enables us to improve modern standards of healthcare – not only on a local but also on a global level. Some examples of current WHATs are migrant health, mobile populations, changing environments, disease spread – communicable and non-communicable and digitization. We understand Interconnected care as the HOW, a concept that teaches us how to use what we have in order to improve the outcome when the situation is complex and dynamic. It is therefore crucial for stakeholders to sit down together, taking enough time to get familiar and connect over the issue before suggesting possible solutions. This means to think about how and with whom to get connected and have a clear identification and description of the WHAT before deciding how to tackle it. This will result in a practical map and the common knowledge of how to use and read it.
If the situation is static or very clear then linear approaches are still the chosen approach – the most use example here is the tackling of Acute medical conditions.
To give you an overview on how diverse interconnected care can or could be, we would like to describe two examples in the following:
In light of the aforementioned, we can then reframe our view on healthcare and think about Systems Thinking in a more dynamic manner. As a self-organized system where we need to be aware of the possibilities that lie in each part.
Interconnected care includes:
HOW DOES THIS AFFECT CHILDREN AND WHAT SHOULD BE DONE?
Pediatric patients often come along with diverse challenges, interests and needs due to the colorful interaction between their families, their social environment and their individual needs that all have to be addressed equally and underline the importance of a more holistic and interconnected approach. Children of today grow up in an increasingly globalized, moving world with mobile populations and a high level of interconnectivity between people living on different continents of the world. These circumstances all come along with different challenges in healthcare that can best be addressed by Interconnected care. From a child’s perspective it must therefore only be sensible to establish the concept of Interconnected care in healthcare.
Especially with rare diseases Interconnected care becomes inevitable in the light of the often small numbers of patients with one condition that emphasizes the need for close cooperation, the exchange of knowledge and experience and synergies in research.
Topics that should also be addressed by the concept of interconnected care are prevention and public health matters. Prevention starts with conception, continues its way during pregnancy when fetal programming is creating the first influential environment for later life and is of great importance for every human being for example in order to avoid unnecessary chronic conditions, identify and contain future outbreaks of communicable diseases.
Another under-represented area of healthcare is the public health sector that would also benefit from more interconnectivity, thereby helping to provide better patient and community-centered care – and not only in a pandemic as we are facing it at the moment. A steadier utilization and distribution of resources could be a result from vivid interconnectivity among stakeholders.
OUR RECOMMENDATIONS
In order to bring Interconnected care into practice we summarize our main recommendations in the following:
About the authors:
List of Authors
Lena de Maizière represents the German pediatric trainees within Young EAP. She is a 4th year paediatric resident.
Karen Daehlin Holm represents the Norwegian pediatric trainees within Young EAP. She is a 3rd year pediatric resident, currently doing a year side-specializing in child- and youth mental health.
References

New ways to test high-risk medical devices.
Manufacturers of medical devices need to test their products before being allowed to market them. Specifically, they require clinical data showing their medical device is safe and efficient. In this context, the EU-funded CORE-MD project will translate expert scientific and clinical evidence on study designs for evaluating high-risk medical devices into advice for EU regulators. The project will propose how new trial designs can contribute and suggest ways to aggregate real-world data from medical device registries.
It will also conduct multidisciplinary workshops to propose a hierarchy of levels of evidence from clinical investigations, as well as educational and training objectives for all stakeholders, to build expertise in regulatory science in Europe. CORE–MD will translate expert scientific and clinical evidence on study designs for evaluating high-risk medical devices into advice for EU regulators, to achieve an appropriate balance between innovation, safety, and effectiveness. A unique collaboration between medical associations, regulatory agencies, notified bodies, academic institutions, patients’ groups, and health technology assessment agencies, will systematically review methodologies for the clinical investigation of high-risk medical devices, recommend how new trial designs can contribute, and advise on methods for aggregating real-world data from medical device registries with experience from clinical practice The consortium is led by the European Society of Cardiology and the European Federation of National Associations of Orthopaedics and Traumatology, and involves all 33 specialist medical associations that are members of the Biomedical Alliance in Europe.

