Childhood obesity is one of the most serious public health challenges of the 21st century. Last year, the Commission on Ending Childhood Obesity (ECHO) reported that the number of obese children and adolescents globally has increased tenfold in the last 40 years. In 2016, an estimated 41 million children under 5 years of age were affected by overweight or obesity. An even greater number of children are, even from birth, on the pathway to developing obesity. In absolute numbers, more overweight and obese children live in low- and middle-income countries than in high-income countries. Within countries, certain subgroups such as children from migrant and indigenous groups and from socioeconomically disadvantaged families are at a particularly high risk of becoming obese due to rapid acculturation and poor access to public health information.
Current situation
The overall worldwide prevalence of childhood obesity increased eightfold since 1975. According to World Health Organisation (WHO) statistics, in the WHO European Region today 30 – 70% of adults are overweight, and 10 – 30% are obese. A concerning statistic is that more than 60% of children who are overweight before puberty will be overweight as adults. According to the latest data from WHO Childhood Obesity Surveillance Initiative (COSI), childhood obesity rates in the southern European countries are among the highest in the world. Between 2015 and 2017, childhood obesity rates were highest in Cyprus, Greece, Italy, Malta, San Marino and Spain where approximately one in five boys were found to be obese (18%-21% of boys). Rates of obesity among girls were slightly lower. These data were presented at the European Congress on Obesity in Vienna last month.
Today, as standards of living continue to rise, weight gain and obesity are posing a threat to health. Dr João Breda, head of the WHO European Office for Prevention and Control of Noncommunicable Diseases, has pointed out that a child with obesity is five to seven times more likely to be obese in adulthood compared to those children who are not obese. This has a negative impact on health outcomes. Obesity is a chronic disease in itself and is also a key factor in the natural history of other chronic and noncommunicable diseases, and in young adults it leads to a loss of 12 to 19 healthy life years.
Obesity is a major contributor to ill health worldwide. It is a known risk factor for cardiovascular disease, orthopaedic issues and other significant morbidity, and is also responsible for the increasing incidence of type 2 diabetes amongst children. This in turn is associated with a higher chance of premature death and disability. Moreover, obesity can have an important impact on the psychological state of adolescents when faced with bullying and dealing with self-image issues.
Rapid social and economic development has changed the environment that children are growing up in. Children and families opt for processed foods, high energy dense foods and increased intake of sugars including sugary drinks. Whilst ‘sugar taxes’ go some way to targeting consumption of unhealthy products, 87% of unhealthy food that children eat is not covered by this. Good marketing of unhealthy food options is an important factor. Only 1.2% of food advertising in the UK focusses on fruits and vegetables, and vegetable sales are in decline.
An increase in sedentary lifestyles from watching television and using electronic media contributes to obesity in childhood. A task force from the European Academy of Paediatrics and the European Childhood Obesity Group recently found that there is evidence of a strong link between obesity levels across European countries and childhood media exposure. The task force recommends that paediatricians routinely ask parents and adolescents about the family’s use of mass media, inform them about the general risks, educate them on how to use social media safely and ensure that they understand the importance of adhering to guidelines for a healthy diet, adequate physical activity and sleep.
It was observed from the COSI report that despite the high rates recorded in the period 2015 – 2017, a significant decrease in the prevalence of obesity was recorded over the last 10 years in Greece, Italy, Portugal, Slovenia, Ireland and Spain. This encourages us. Despite the fact that there is still a long way to go in defeating this ‘pandemic’ called obesity, there is indeed much hope for improvement if paediatricians, authorities, policy makers and families, all work together for a better and healthier lifestyle. Paediatricians play a lead role in advocating for the rights of children to access healthy food and drinks and an active lifestyle, and to be protected from the harmful effects of advertising and marketing. Establishing healthy behaviors at an early age allows children to develop a healthy growth trajectory. This asks for an approach across sectors and across the life course.
What Young EAP do
By raising awareness of the issue, young EAP urges paediatricians and other healthcare providers to identify and manage children who are (at risk of becoming) overweight or obese. In addition, preventive counselling should begin during preconception, and continue during infancy, and focus on healthy feeding, activity and family lifestyle behaviors. Techniques like motivational interviewing can be used to achieve healthy lifestyle modifications and should be trained during core paediatric training.
Young EAP also invites policy and decision makers together with healthcare authorities to reflect upon both the ill-effects and the financial burden of obesity and its complications. We encourage policy makers to invest in pro-health initiatives and in incentives within schools and families to prevent childhood obesity. In light of the increase in population density in some countries, one way to do this is to invest more in safe outdoor spaces for physical activity for children and families. Furthermore, as children spend a substantial amount of time at school, an increase of the allocated time for physical activity, standards for healthy food options, and elimination of sugar containing drinks from preschools and schools could have a significant impact on children making healthy choices. In addition, measures are required to facilitate making the healthier choice the easier choice, such as simple front-of-pack labelling of food products based on nutritional profiles, and restriction of advertising of food products to children. It is important that improvements are made across all sectors, including schools, home, health care, the food industry, communities and the public sector.
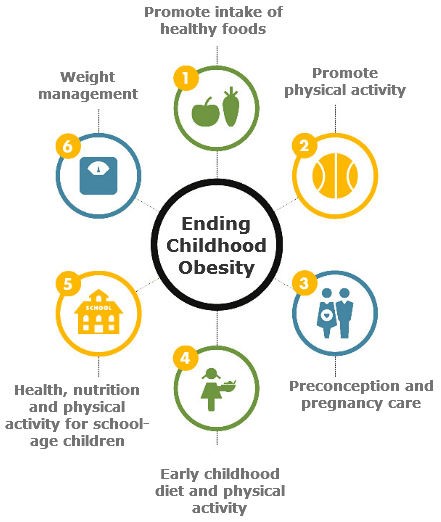
(Image Source: Recommendations of the Commission on Ending Childhood Obesity, European Commission)
About the authors:
List of Authors
Sian Copley is a 3rd year resident from the UK working in the North East of England and representing UK paediatric trainees within Young EAP and paediatric trainees/Young EAP within the EAP Advocacy Group.
Lenneke Schrier is the European Junior Doctor Representative to the European Academy of Paediatrics, and the Chair of Young EAP. She is a 4th year paediatric trainee at the Leiden University Medical Center in the Netherlands.
Veronica Said Pullicino is a 4th tear paediatric trainee in Malta, and she represents the Maltese paediatric trainees within the Young EAP.
Berthold Koletzko is a Prof. of Paediatrics at the Ludwig-Maximilians-University of Munich (LMU), a paediatrician at the Children’s Hospital and Children clinic of the Dr. von Hauner Children’s Hospital, and a EAP member.

New ways to test high-risk medical devices.
Manufacturers of medical devices need to test their products before being allowed to market them. Specifically, they require clinical data showing their medical device is safe and efficient. In this context, the EU-funded CORE-MD project will translate expert scientific and clinical evidence on study designs for evaluating high-risk medical devices into advice for EU regulators. The project will propose how new trial designs can contribute and suggest ways to aggregate real-world data from medical device registries.
It will also conduct multidisciplinary workshops to propose a hierarchy of levels of evidence from clinical investigations, as well as educational and training objectives for all stakeholders, to build expertise in regulatory science in Europe. CORE–MD will translate expert scientific and clinical evidence on study designs for evaluating high-risk medical devices into advice for EU regulators, to achieve an appropriate balance between innovation, safety, and effectiveness. A unique collaboration between medical associations, regulatory agencies, notified bodies, academic institutions, patients’ groups, and health technology assessment agencies, will systematically review methodologies for the clinical investigation of high-risk medical devices, recommend how new trial designs can contribute, and advise on methods for aggregating real-world data from medical device registries with experience from clinical practice The consortium is led by the European Society of Cardiology and the European Federation of National Associations of Orthopaedics and Traumatology, and involves all 33 specialist medical associations that are members of the Biomedical Alliance in Europe.

